Metabolic Health
Secondary Iron Overload: Transfusions, Anemias, and Parenteral Iron
Acquired iron excess from transfusions, ineffective erythropoiesis, or IV iron—not classic HFE hepcidin failure. Phlebotomy often fails when anemia is present.
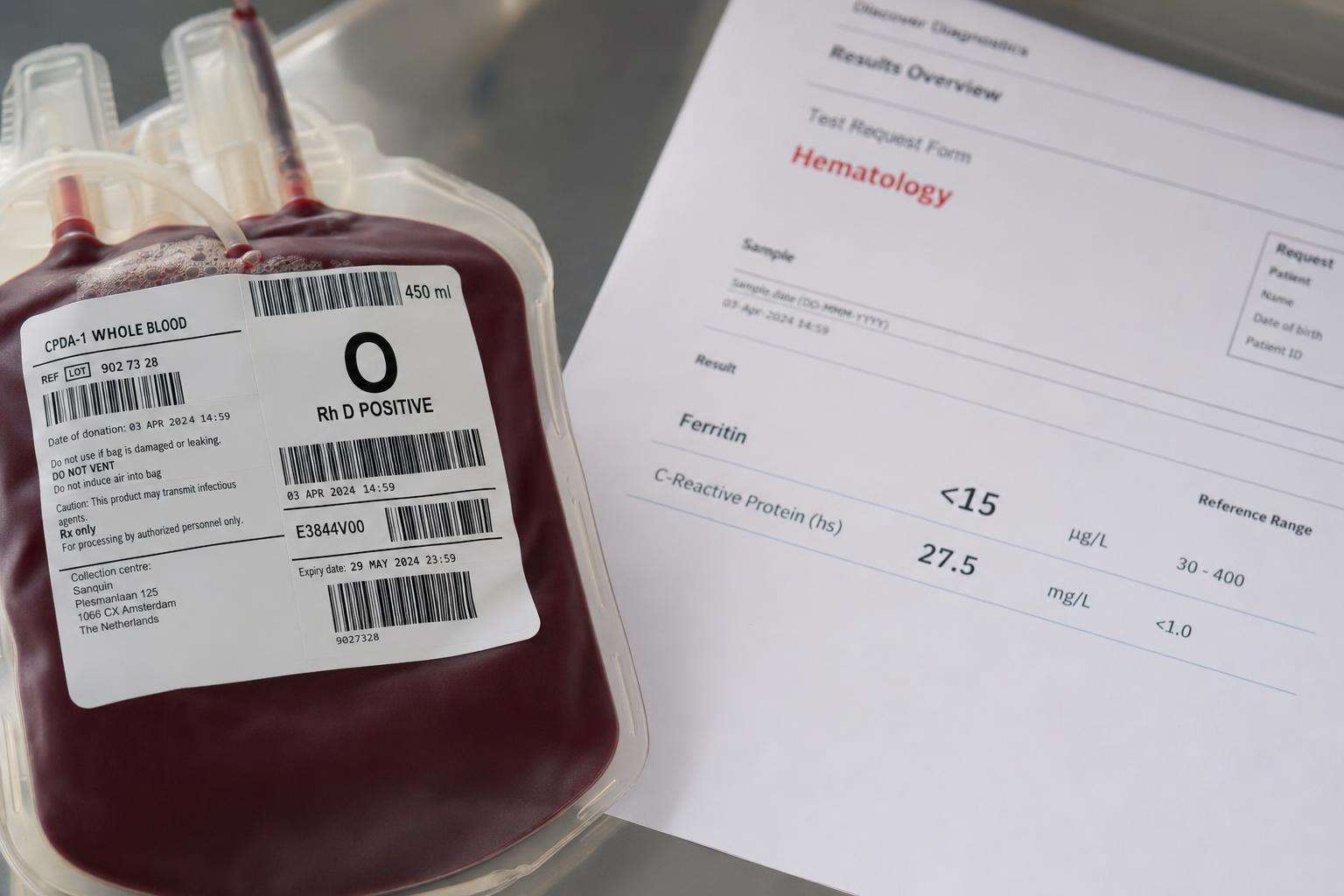
Secondary iron overload is acquired excess iron—transfusions, iron-loading anemias, IV iron—not classic HFE hepcidin failure. Each RBC unit deposits ~200–250 mg iron. If the patient is anemic, chelation usually beats phlebotomy. Do not brand every high ferritin as genetic hemochromatosis.
High ferritin is a common lab finding. The wrong next story—calling every elevation hereditary hemochromatosis—sends patients down genetic pathways that miss transfusions, parenteral iron, and liver-disease redistribution.
This article is informational and editorial only. It is not medical advice, diagnosis, or a treatment plan. Numbers and literature ranges cited here are not personal prescriptions. Consult a qualified clinician before changing medications, supplements, diet, equipment, or management of a diagnosed condition. Seek urgent care for emergencies.
What causes secondary iron overload?
The AASLD hemochromatosis guideline divides overload into inherited HFE-related disease, secondary overload, and rarer miscellaneous disorders. Secondary causes include thalassemia major, sideroblastic anemia, chronic hemolysis, aplastic anemia, repeated red-cell transfusions, iron–dextran and other parenteral iron, long-term dialysis contexts, and iron redistribution patterns in HCV, HBV, alcoholic liver disease, NAFLD, and porphyria cutanea tarda.
Oral diet alone is a weak overload driver without ineffective erythropoiesis or genetic predisposition. Parenteral iron and transfusions inject iron past gut regulation. Source accounting starts with cumulative units: units times roughly 200–250 mg iron estimates exogenous load before any genetics discussion. That arithmetic alone can explain multi-gram stores after years of chronic transfusion support.
Chronic inflammation and NAFLD can raise ferritin without multi-gram parenchymal iron. That is hyperferritinemia with a different risk and treatment map—treat the liver disease and metabolic drivers rather than automatically launching weekly phlebotomy or unregulated chelation products sold online as detox.
How do histology and clinical patterns differ from HFE HH?
Classic hereditary hemochromatosis loads hepatocytes via excess absorption from low hepcidin tone. Secondary and many transfusional states more often load Kupffer cells and macrophages first. AASLD teaching materials use that compartment pattern to avoid forcing every high-iron biopsy into the HFE narrative when the chart already lists dozens of units transfused over years of care.
Clinically, secondary cases live inside hematology clinics: transfusion logs, erythropoietin use, and cardiac iron risk in multi-transfused patients. Primary HFE cases often present later with fatigue, joint pain, liver enzyme changes, or endocrine findings after years of silent absorption. Both can damage organs; the unloading tool differs sharply between pathways.
| Feature | Classic HFE HH | Secondary overload |
|---|---|---|
| Main driver | Absorption (hepcidin) | Transfusions / parenteral / dyserythropoiesis |
| Typical iron cell | Hepatocytes | Often Kupffer/macrophage |
| Phlebotomy | First-line if Hb allows | Often unsuitable if anemic |
| Chelation | Special cases | Common first-line path |
| Family genetics | Cascade HFE testing | Usually not the primary story |
When is chelation preferred over phlebotomy?
Ask one gate question: can this patient safely lose red cells? If transfusion-dependent or significantly anemic, serial therapeutic phlebotomy is usually the wrong tool. Reviews of secondary hemochromatosis due to hereditary or acquired anemia state that phlebotomy is not suitable and chelation is used instead. The CDC likewise notes iron chelation when blood removal is not possible for practical clinical reasons.
Transfusional programs monitor organ iron with liver and cardiac MRI strategies under hematology protocols. Deferoxamine historical dose bands in AASLD tables (example 20–40 mg/kg/day for dyserythropoietic secondary overload) and oral agents such as deferasirox require toxicity monitoring—never unsupervised detox chelation marketed on social media without labs or organ imaging.
Contemporary hematology reviews of iron overload management stress lessons from transfusion programs: match intensity of unloading to organ risk, not to wellness trends. Cardiac T2* and liver iron concentration are decision tools, not optional boutique extras for the curious patient only.
What workup mistakes are most common?
Common failure modes include weekly phlebotomy blogs applied to transfusion-dependent patients; calling a post–IV-iron ferritin spike genetic hemochromatosis; ignoring cumulative transfusion counts; equating NAFLD-associated ferritin rise with multi-gram transfusional siderosis; and stopping after a negative HFE test when the real issue was never genetic absorption in the first place.
ACG-style guidance synthesized in AASLD educational material: exclude secondary causes when overload is suspected without C282Y homozygosity. Genetics still matter when phenotype could be primary—but transfusion history is a laboratory result. For mild iron in chronic liver disease, treat the liver disease rather than escalating unloading without quantified stores.
What should patients and clinicians do next?
Inventory iron inputs including transfusions, IV iron, and supplements. Order a full iron panel with clinical context, not ferritin alone. Image or stage the liver when indicated. Refer multi-transfused or anemic patients to hematology for chelation programs with organ-specific monitoring. Screen families only when hereditary disease remains plausible after secondary causes are cleared or documented as coexisting problems.
Secondary overload is highly treatable when named correctly. Mislabeling it as just hemochromatosis or just inflammation both delay the right lever—chelation, modified transfusion strategy, stopping unnecessary parenteral iron, or targeted phlebotomy when hemoglobin safely allows serial units over a planned induction course.
Editorial note: ranges and protocol bands cited here are literature and guideline context for shared decision-making with clinicians—not self-directed treatment schedules, home lab targets, or substitute care for emergencies or progressive organ disease.
Sources & citations
Frequently asked