Metabolic Health
Reading an Iron Panel: Step by Step (2026)
Read ferritin with TSAT, separate inflammation from overload, know when HFE genetics help, and avoid ferritin-only panic.
ferritinTSATHFEanemiaoverload
Bottom line
Ferritin+TSAT, inflammation, genetics only when indicated—no portal panic.
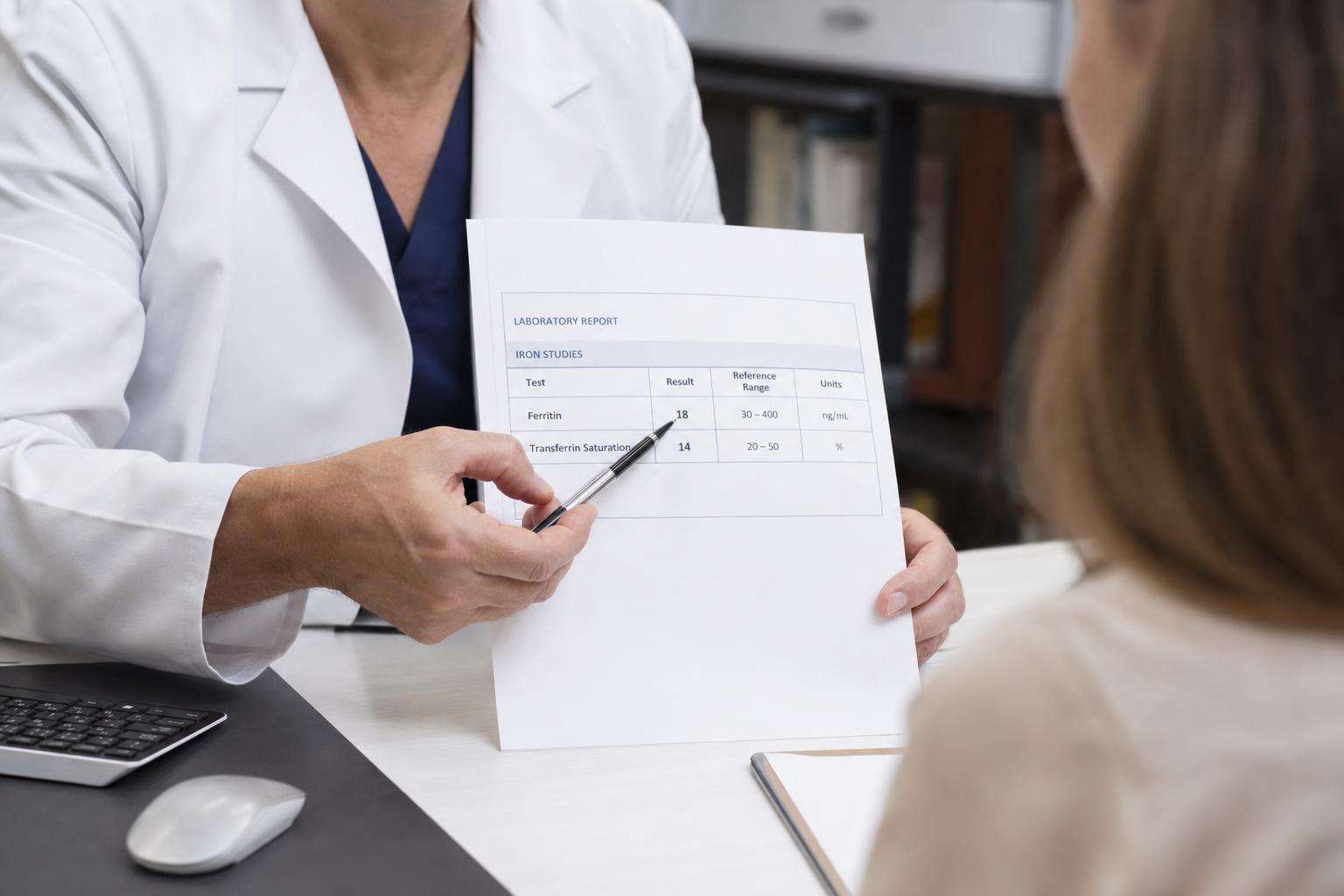
- Always read ferritin with transferrin saturation — TSAT helps separate iron overload patterns from many high-ferritin inflammatory states.
- Screen for inflammation and alcohol/liver context — Often explains high ferritin without expensive genetics—using history and basic labs you may already have.
- Follow overload workup path (consider HFE/specialty) — That pattern raises hereditary hemochromatosis probability and needs structured evaluation, not iron pills.
How we built this guide
Ranked interpretation steps by error prevention (especially iron pills in overload), marker pairing, and guideline-aligned escalation.
- Dose / clinical impact. Likely effect on exposure or health decision quality.
- Evidence base. Agency guidance, trials, or consensus statements.
- Adherence cost. Money, time, and household friction.
- Harm of misuse. Whether bad execution creates new risks.
Key takeaways
- Always pair ferritin with transferrin saturation (TSAT)
- Read high ferritin against inflammation and liver factors
- Work up iron deficiency as a cause-finding process
- Escalate suspected iron overload on a structured path
- Use HFE genetics when the pattern indicates, not as a wellness panel
- Set recheck intervals and treatment-response criteria
Always pair ferritin with transferrin saturation (TSAT)
One number is not a panel
Who this is for: Anyone reading outpatient iron results
Do
- Prevents ferritin-only misreads
- Separates common inflammatory patterns
- Cheap incremental labs when missing
- Blocks inappropriate iron pills
Watch out
- Reference ranges vary; fasting/compliance affect iron/TIBC
Read high ferritin against inflammation and liver factors
Fatty liver and alcohol commonly raise ferritin
Who this is for: Patients with isolated high ferritin and metabolic risk
Do
- Explains many high-ferritin cases cheaply
- Uses history patients can provide
- Reduces unnecessary genetics
- Integrates liver metabolic workups
Watch out
- Can delay overload diagnosis if pattern ignored; history may be incomplete
Work up iron deficiency as a cause-finding process
Low stores are a clue, not a multivitamin ad
Who this is for: Low ferritin, iron-deficiency anemia, or high-risk bleeding groups
Do
- Connects labs to actionable causes
- Prevents missed GI pathology
- Structures repletion and recheck
- Discourages wellness iron misuse
Watch out
- Workups can be invasive; side effects limit oral iron
Escalate suspected iron overload on a structured path
High ferritin + high TSAT is not a gym supplement cue
Who this is for: High ferritin with elevated TSAT or known family hemochromatosis
Do
- Safety-critical branch for overload
- Links to genetics and family counseling
- Opens phlebotomy pathways correctly
- Stops dangerous self-supplementation
Watch out
- Incomplete penetrance confuses patients; specialist access varies
Use HFE genetics when the pattern indicates, not as a wellness panel
Genotype is not a fitness score
Who this is for: Biochemically suggestive cases or first-degree relative cascades
Do
- Reduces recreational genetics waste
- Focuses counseling on high-yield cases
- Supports cascade family testing
- Avoids DTC misreads
Watch out
- Access and counseling quality vary; non-HFE disease exists
Set recheck intervals and treatment-response criteria
One lab is a snapshot
Who this is for: Anyone starting iron therapy or overload monitoring
Do
- Converts snapshots into trajectories
- Catches nonresponse early
- Documents therapy effects
- Reduces one-off portal panic
Watch out
- Interval uncertainty; adherence to follow-up is hard
Frequently asked
Can ferritin be high without iron overload?
Yes. Ferritin rises with inflammation, infection, alcohol use, and common liver conditions such as fatty liver. Transferrin saturation and clinical context help separate these patterns from iron overload. Do not start iron supplements based on high ferritin alone. Confirm details with a qualified clinician or primary guidance document when your situation is high-stakes.
What TSAT level is concerning for hemochromatosis?
Clinicians often pay attention to sustained elevated transferrin saturation alongside high ferritin, with exact thresholds and fasting conditions depending on lab and guideline context. A single mildly abnormal value needs confirmation. High TSAT with high ferritin warrants medical evaluation, not self-phlebotomy.
Should I take iron if I am tired and ferritin is normal?
Usually no. Fatigue has many causes. Extra iron when stores are adequate can be harmful, especially if undiagnosed overload exists. Ask for a proper workup rather than using iron as a generic energy supplement. Confirm details with a qualified clinician or primary guidance document when your situation is high-stakes.
Is HFE testing recommended for everyone?
No. It is most useful when iron studies suggest overload or when a close relative has hereditary hemochromatosis. Routine wellness genotyping without biochemical indication creates counseling noise and is not a substitute for iron panels. Confirm details with a qualified clinician or primary guidance document when your situation is high-stakes.
Can I treat high ferritin by donating blood on my own?
Do not replace medical care with unsupervised donation. If phlebotomy is indicated for iron overload, it should be clinician-directed with target ferritin/TSAT goals and liver risk assessment. Donation eligibility rules also differ from therapeutic phlebotomy protocols. Confirm details with a qualified clinician or primary guidance document when your situation is high-stakes.