Light & Recovery
UVA vs UVB: Spectrum, Skin Biology, Vitamin D, Photoaging, and Cancer
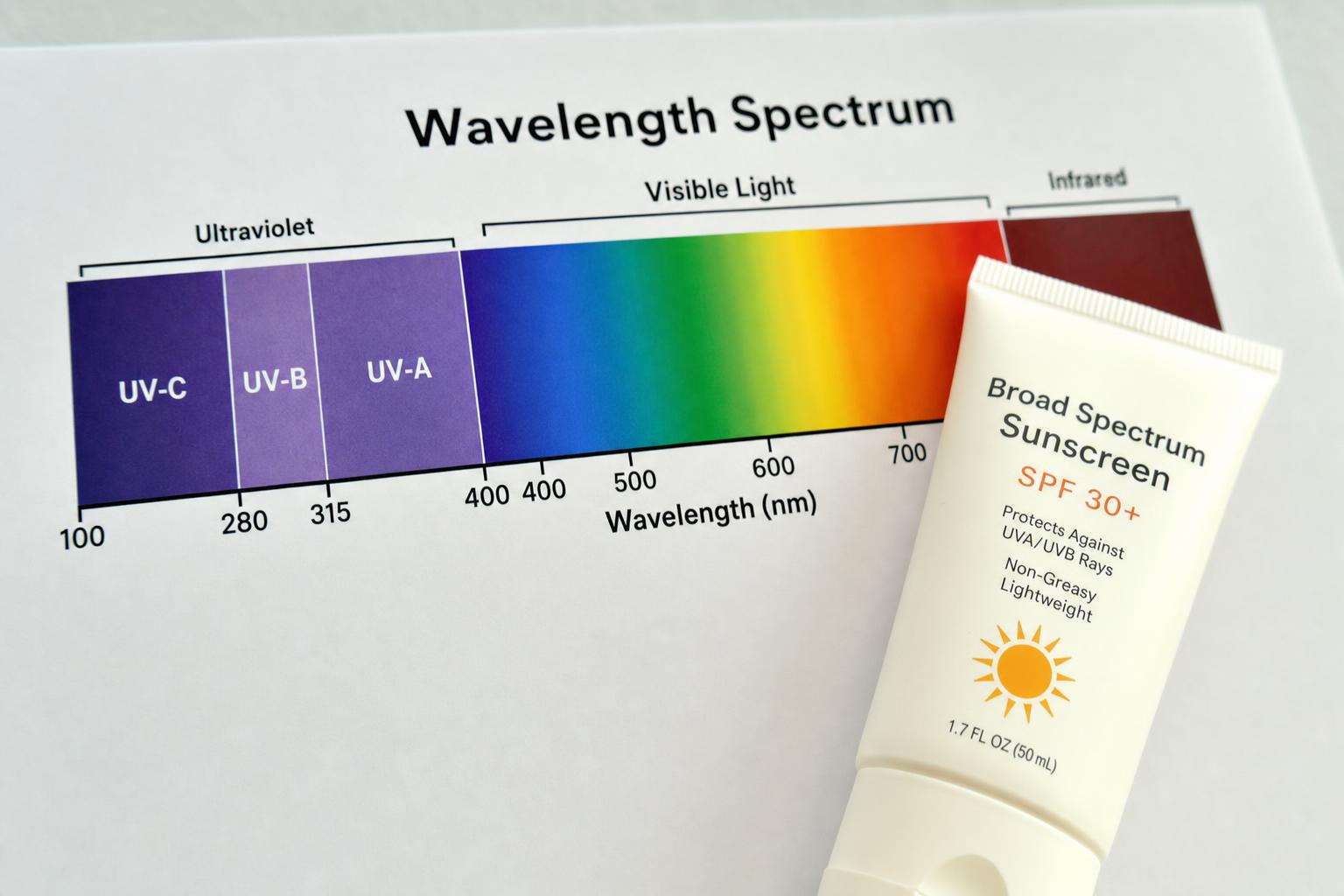
UVB (~280–315 nm): sunburn, CPDs, vitamin D. UVA (~315–400 nm): deeper dermal ROS, photoaging, NO stores. Both contribute to carcinogenesis. Visible light drives ocular circadian effects.
UVB: burn + vitamin D + direct DNA photoproducts. UVA: deeper ROS photoaging + NO stores research. Both → cancer risk pathways. Visible light → eyes/circadian. Broad-spectrum protection is rational.
If you cannot map wavelength bands, you will mishandle every sunlight debate—from sunscreen to nitric oxide tweets to window offices.
This article is informational and editorial only. It is not medical advice, diagnosis, or a treatment plan. Numbers and literature ranges cited here are not personal prescriptions. Consult a qualified clinician before changing medications, supplements, diet, equipment, or management of a diagnosed condition. Seek urgent care for emergencies.
What are the standard UV bands at Earth’s surface?
UVB ~280–315 nm (small fraction, high biological punch).
UVA ~315–400 nm (majority of terrestrial UV).
UVC filtered by ozone—not a casual outdoor band.
How does biology split by band?
UVB: erythema, CPDs/6-4PPs, previtamin D3.
UVA: dermal penetration, ROS, MMPs, photoaging; experimental dermal NO release linked to BP research (Liu-class studies).
Both: carcinogenesis and immunosuppression pathways.
| Band | Skin hallmark | Health note |
|---|---|---|
| UVB | Burn + CPDs + D3 | Small fraction, high impact |
| UVA | Photoaging ROS | Windows still transmit |
| UVA+UVB | Cancer pathways | Group 1 solar radiation |
| Visible | Circadian eyes | Not vitamin D |
| Sunbeds | Often UVA-rich | Avoid for D |
What protection implications follow?
Broad-spectrum sunscreen (UVA+UVB), clothing, shade—especially when UVI ≥3.
Window glass: UVA aging without D benefit.
Tanning beds often UVA-heavy and classified carcinogenic—avoid.
What benefit map stays honest?
UVB→D (with burn co-risk).
UVA→experimental vascular NO (not a tanning indication).
Visible outdoor light→circadian/mood via eyes.
None require intentional erythema.
Sources: WHO UV radiation; Engelsen UV vitamin D; Photoaging mechanisms review context.
Readers should dual-source primary literature, translate slogans into exposure units and effect sizes, and rank interventions by expected value under uncertainty. Cheap reversible steps often outrank extreme protocols. Opportunity cost is real: hours spent on unvalidated tests are hours not spent on sleep, training, protein adequacy, and primary care. Sex, life stage, comorbidities, medications, and geography change interpretation. Prefer falsifiable claims with named endpoints over multi-disease cure lists. Update beliefs when stronger trials appear rather than freezing identity around a single paper or influencer narrative. Measured curiosity beats both panic and complacency. Further reading should prioritize primary sources and consensus documents over secondary social summaries. When evidence is mixed, state both the signal and the limits in the same paragraph. When evidence is strong, still avoid overclaiming universality across populations.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Sources & citations
Frequently asked