Light & Recovery
Latitude, Season, and UV Index: When Sunlight Makes Vitamin D—and When It Does Not
Vitamin D winter is real at high latitudes. UVI guides burn protection (≥3). Bright visible light ≠ adequate UVB for cutaneous D3.
Vitamin D winter is latitude×season physics. UVI ≥3 → protect skin. Bright skies ≠ UVB for D. Midday maximizes both D potential and burn risk together.
Geography is a medical variable. The same lunch walk that raises 25(OH)D in June at 30°N may do almost nothing for D in December at 50°N—while still glaring brightly through clouds of visible light.
This article is informational and editorial only. It is not medical advice, diagnosis, or a treatment plan. Numbers and literature ranges cited here are not personal prescriptions. Consult a qualified clinician before changing medications, supplements, diet, equipment, or management of a diagnosed condition. Seek urgent care for emergencies.
What physical drivers set UVB dose?
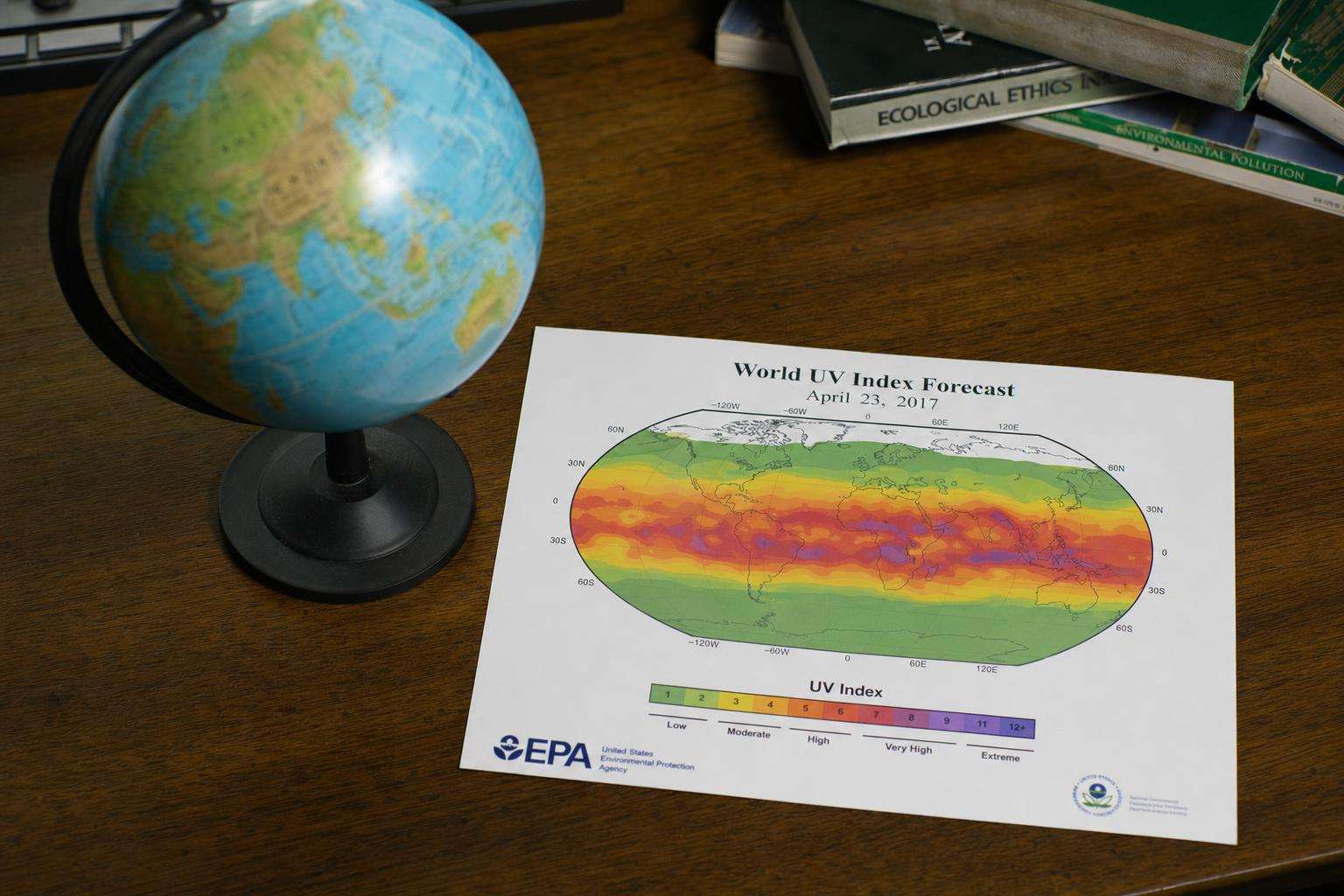
Solar elevation (latitude, season, time of day), ozone column, clouds, altitude, surface reflectance.
Shortwave UVB is preferentially depleted at low sun angles.
Equator higher year-round potential; poles extreme winters.
How should UVI be used day to day?
Check local forecast; protect at ≥3; reapply sunscreen as directed for outdoor work/sport.
Sunscreen is not for intentional burn extension.
Eye protection matters at high albedo (snow, water).
| Factor | UVB effect | Action |
|---|---|---|
| High latitude winter | ↓↓ D synthesis | Oral D / diet |
| Midday summer | ↑ UVB + burn | Short + protect |
| UVI ≥3 | Harm risk | Shade/clothes/SPF |
| Snow albedo | ↑ exposure | Eyes + face care |
| Thick clouds | ↓ UVB | Don’t assume zero burn |
What historical photobiology findings matter?
Winter sunlight in some northern cities historically failed to promote cutaneous D3 (Webb/Holick lineage).
Engelsen reviews global low status patterns across latitudes and skin types.
Deeply pigmented skin at high latitude needs oral D consideration more often.
What practical calendar rule helps?
Summer: brief unprotected daylight can contribute D for many—still avoid burns.
Winter high latitude: prioritize oral D per guidelines + daylight for circadian eyes.
Never use tanning beds for D.
Sources: WHO ultraviolet radiation fact sheet; Engelsen 2010 vitamin D UV; Young 2021 sunlight vitamin D context.
Readers should dual-source primary literature, translate slogans into exposure units and effect sizes, and rank interventions by expected value under uncertainty. Cheap reversible steps often outrank extreme protocols. Opportunity cost is real: hours spent on unvalidated tests are hours not spent on sleep, training, protein adequacy, and primary care. Sex, life stage, comorbidities, medications, and geography change interpretation. Prefer falsifiable claims with named endpoints over multi-disease cure lists. Update beliefs when stronger trials appear rather than freezing identity around a single paper or influencer narrative. Measured curiosity beats both panic and complacency. Further reading should prioritize primary sources and consensus documents over secondary social summaries. When evidence is mixed, state both the signal and the limits in the same paragraph. When evidence is strong, still avoid overclaiming universality across populations.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims.
Sources & citations
Frequently asked