Hormones & Genes
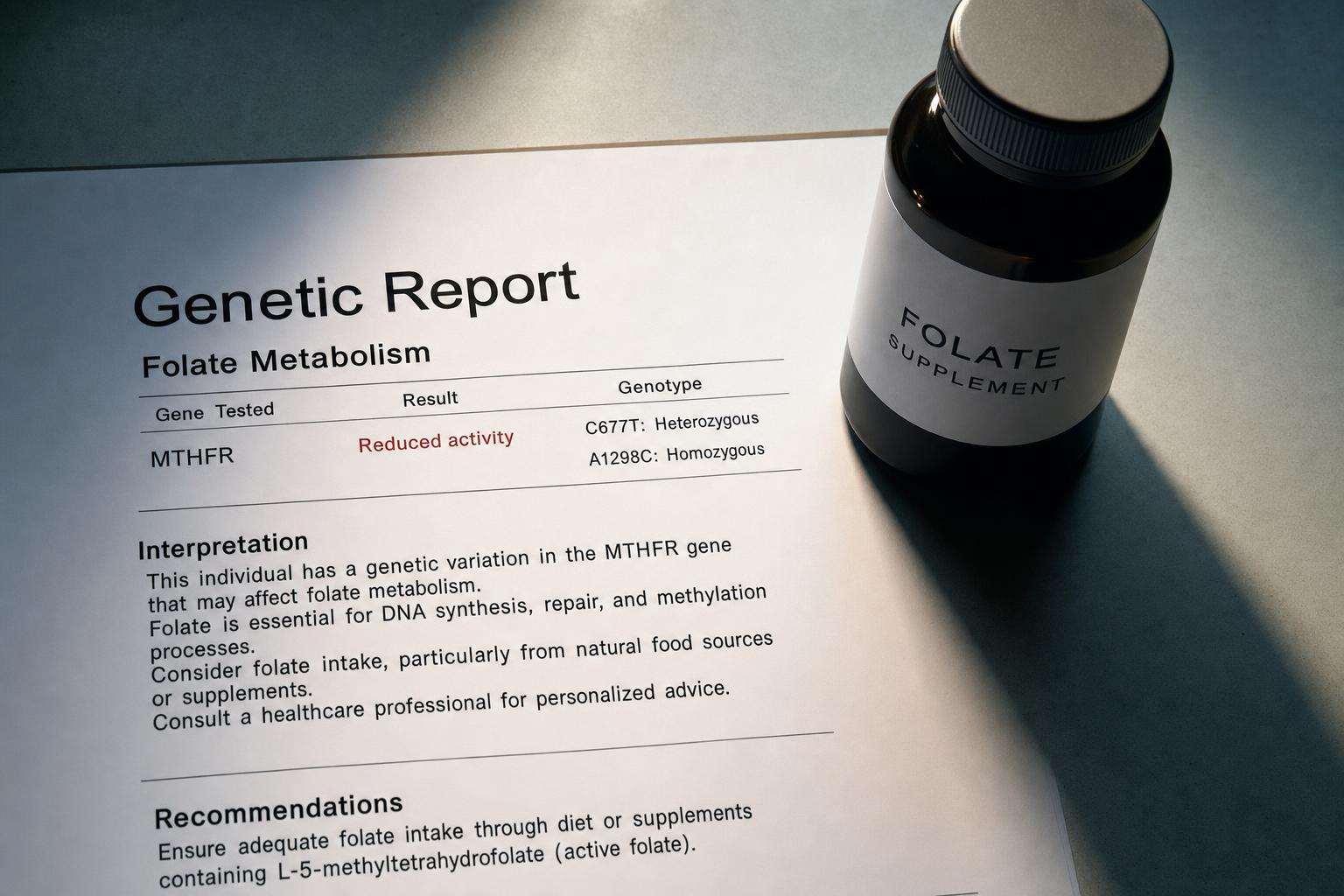
MTHFR in Functional Medicine vs ACMG Framing: Two Different Languages
ACMG cautions against routine MTHFR SNP testing for common indications. Functional-medicine marketing often expands SNPs into multi-system narratives. Know which frame you are in.
ACMG-class framing: don’t routine-test common MTHFR SNPs for many indications. Functional marketing: often expands SNPs into protocols. Keep Grade A folic acid NTD prevention above merch narratives.
MTHFR arguments fail when people debate brands of folate without noticing they are using incompatible evidence rules.
This article is informational and editorial only. It is not medical advice, diagnosis, or a treatment plan. Numbers and literature ranges cited here are not personal prescriptions. Consult a qualified clinician before changing medications, supplements, diet, equipment, or management of a diagnosed condition. Seek urgent care for emergencies.
What is load-bearing in mainstream genetics?
Variant frequency, penetrance, clinical utility of testing, and proven interventions.
Severe enzymatic deficiency ≠ heterozygous common SNPs.
Homocysteine interpretation needs clinical context.
What is load-bearing in functional marketing?
Patient narrative coherence, supplement personalization, and distrust of “synthetic” folic acid.
These can help engagement—and also overfit noise.
Commercial incentives for testing + supplements are structural.
| Question | ACMG-class lean | Functional lean risk |
|---|---|---|
| Routine SNP test? | Generally no | Often yes/upsell |
| NTD prevention | Folic acid evidence | Sometimes form debates |
| Symptom attribution | Narrow | Broad methylation story |
| Utility bar | Changes management | Narrative fit |
Where does patient harm appear?
Skipping folic acid preconception; over-supplementation; anxiety from over-interpreted SNPs; missed real diagnoses.
Opportunity cost versus sleep, diet pattern, and indicated medical care.
Thrombophilia mismanagement if SNPs replace proper workups.
What is a sane synthesis?
No routine MTHFR SNP shopping for vague symptoms.
Follow pregnancy folate guidance; investigate true deficiencies.
Use genetics clinics for complex cases—not multi-level marketing panels.
Sources: ACMG genetics guidance hub; CDC folic acid; GeneReviews MTHFR context.
Readers should dual-source primary literature, translate slogans into exposure units and effect sizes, and rank interventions by expected value under uncertainty. Cheap reversible steps often outrank extreme protocols. Opportunity cost is real: hours spent on unvalidated tests are hours not spent on sleep, training, protein adequacy, and primary care. Sex, life stage, comorbidities, medications, and geography change interpretation. Prefer falsifiable claims with named endpoints over multi-disease cure lists. Update beliefs when stronger trials appear rather than freezing identity around a single paper or influencer narrative. Measured curiosity beats both panic and complacency. Further reading should prioritize primary sources and consensus documents over secondary social summaries. When evidence is mixed, state both the signal and the limits in the same paragraph. When evidence is strong, still avoid overclaiming universality across populations. Pattern quality, dose, and adherence dominate most household decisions more than brand seals.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Sources & citations
Frequently asked