Fitness
RPE-Based Autoregulation for Women’s Resistance Training
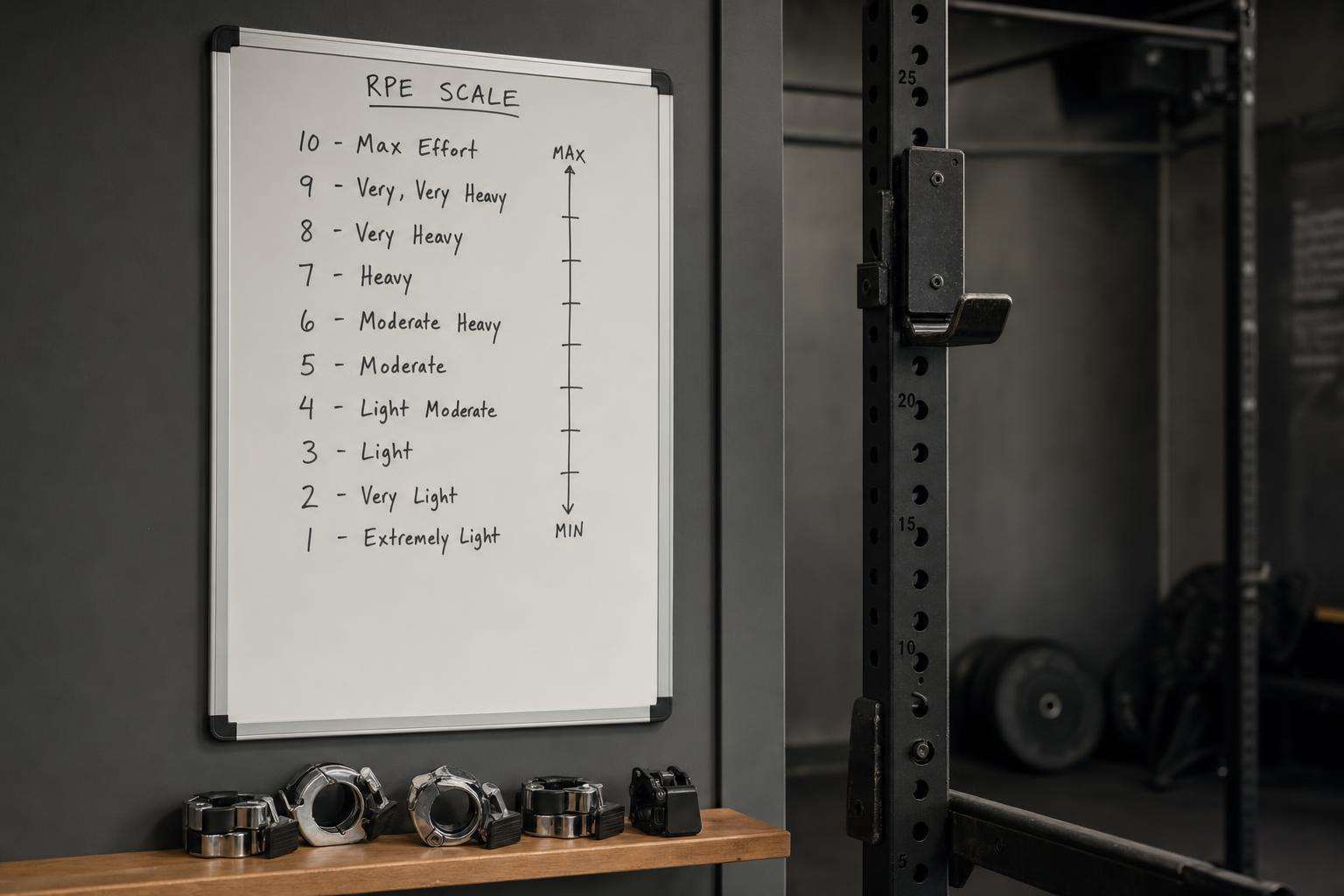
Rate of perceived exertion and reps-in-reserve let women adjust daily readiness without abandoning progression. Learn the scale; log it; progress on good days.
RPE/RIR autoregulation matches daily readiness while preserving progressive overload. Log honestly, recalibrate occasionally, and progress when targets are met—not when the calendar shames you.
Fixed percentage programs assume a body that sleeps, eats, and recovers like a spreadsheet. RPE admits you are an organism.
This article is informational and editorial only. It is not medical advice, diagnosis, or a treatment plan. Numbers and literature ranges cited here are not personal prescriptions. Consult a qualified clinician before changing medications, supplements, diet, equipment, or management of a diagnosed condition. Seek urgent care for emergencies.
How to install RPE in a novice-to-intermediate program?
Teach the scale with examples; use 1–2 sets near controlled high RPE periodically for calibration.
Prescribe ranges (e.g., 3×6–8 @ RPE 7–8) rather than only exact loads.
Log load, reps, and RPE every working set.
What rules convert RPE into progression?
If top sets land easier than prescribed RPE, add weight next session.
If form breaks before target RPE, reduce load and cue technique.
Deload when readiness is chronically poor or performance trends down.
| Signal | Meaning | Action |
|---|---|---|
| RPE < target | Too easy | Add load/reps |
| RPE = target | On track | Hold or micro-progress |
| RPE > target | Too hard / fatigue | Reduce load |
| Form breakdown | Skill/fatigue limit | Regress, don’t ego |
Where does autoregulation fail?
Chronic sandbagging; chronic grinding to failure every set; ignoring pain red flags.
No long-term plan—only daily vibes without progressive targets.
Comparing your RPE 8 to someone else’s ego posts.
How to combine with life stress?
Sleep debt and high work stress often raise true RPE for the same load—believe the signal.
Maintain habit frequency with easier RPE rather than skipping entirely when possible.
Nutrition and protein still power recovery; RPE is not a calorie strategy.
Sources: NSCA training resources; Helms RPE/RIR methods context; ACSM hub.
Readers should dual-source primary literature, translate slogans into exposure units and effect sizes, and rank interventions by expected value under uncertainty. Cheap reversible steps often outrank extreme protocols. Opportunity cost is real: hours spent on unvalidated tests are hours not spent on sleep, training, protein adequacy, and primary care. Sex, life stage, comorbidities, medications, and geography change interpretation. Prefer falsifiable claims with named endpoints over multi-disease cure lists. Update beliefs when stronger trials appear rather than freezing identity around a single paper or influencer narrative. Measured curiosity beats both panic and complacency. Further reading should prioritize primary sources and consensus documents over secondary social summaries. When evidence is mixed, state both the signal and the limits in the same paragraph. When evidence is strong, still avoid overclaiming universality across populations. Pattern quality, dose, and adherence dominate most household decisions more than brand seals.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Context, dose, endpoint, and population must travel together; slogans that drop any of those four are not finished claims. Household decisions should favor reversible experiments with measurable outcomes over identity diets or unvalidated testing cascades.
Sources & citations
Frequently asked